Caries or dental decay in children has been known to exist for many centuries [1]. Early Childhood Caries (ECC) is a chronic, transmissible infectious disease affecting the primary (milk) teeth. It is defined as the presence of one or more decayed, filled or missing tooth surfaces in any primary tooth in a child 71 months of age or younger [2,3]. It can result in considerable suffering, pain, reduction of quality of life of affected children and disfigurement and frequently can compromise their future dentition. The etiology of the condition is a combination of frequent consumption of fermentable carbohydrates as liquids, especially at night, with on-demand breast- or bottle-feeding, oral colonization by cariogenic bacteria (especially mutans streptococci) and poor oral hygiene [4].
In the United Arab Emirates (UAE), ECC is the most common childhood disease. The prevalence of ECC in the UAE has been reported as 93.8% in 5-year-old children [6].
Prevention of ECC can be achieved by the education of prospective and new parents, as well as by the identification of 'high risk' children [7]. Strategies have focused on the individual mother and child by preventing transfer of cariogenic bacteria from mother to her infant, using preventive agents such as fluoride and teaching good oral hygiene practices [8]. Community-based approaches have been attempted. An example of a successful program was reported by Kowash et al [9] which investigated the effect of dental health education provided by trained, non professionals (not dentists) carrying out regular home visits in a low socioeconomic high-caries area in Leeds, UK. The study was able to demonstrate a significantly reduced occurrence of ECC after three years.
The treatment of ECC is very costly, time consuming and in most cases, requires full dental rehabilitation under general anesthesia by a pediatric dentist. Unfortunately, in many countries, even in the developed world, these carious teeth end up being extracted.
This paper provides an updated evidence-based review of ECC. The literature in regards to ECC definition and terminology, aetiology, prevalence, clinical picture and management is discussed. A solution to the continuing problem of ECC is suggested.
Definition and Terminology of ECC ECC has been defined as “the presence of one or more decayed (non-cavitated or cavitated lesions), missing (due to caries) or filled tooth surfaces” in any primary tooth in a child 71 months of age or younger [2,3]. In children younger than 3 years of age, any sign of smooth-surface caries is indicative of severe early childhood caries (S-ECC). From ages three through five, one or more cavitated, missing (due to caries), or filled smooth surfaces in primary maxillary anterior teeth or a decayed, missing, or filled score of ≥4 (age three), ≥5 (age four), or ≥6 (age five) surfaces constitutes S-ECC [10]. Dental decay in infants and young children has several names including: “nursing caries”, “nursing bottle caries”, “nursing bottle syndrome”, baby bottle caries” and “baby bottle tooth decay” [4]. These terms are often used interchangeably in dental literature. They describe the condition and the possible etiological factors of the decay as understood by parents, public and professionals. However, none include the concept of a sweetened pacifier, which may be a significant cause in infants. Tinanoff and O’Sullivan used the term “Early Childhood Caries” which has been introduced in the USA to describe caries in infants and young children. This term has been widely accepted as the correct term by most dental clinicians and educators [11].
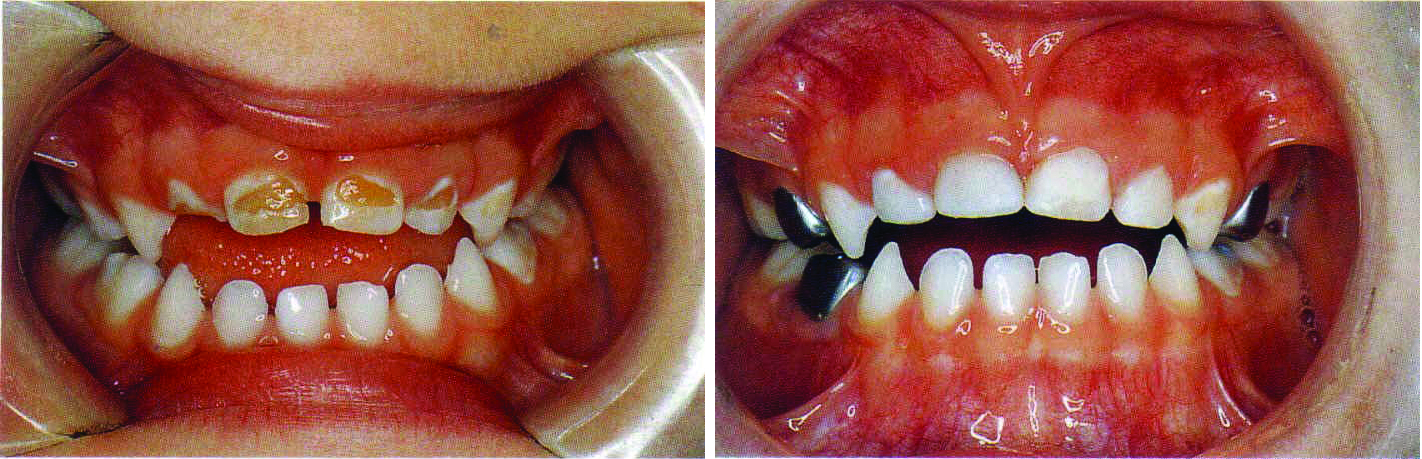
Pattern and Clinical Appearance of ECC ECC has a specific pattern and clinical picture. It is a specific form of rampant caries with the only feature differentiating it from generalized rampant caries being the usual absence of decay of the mandibular incisor teeth (Figure 1). The most commonly affected teeth are the maxillary incisors. Involvement of other teeth (the canines, first and second primary molars) depends on how long the carious process remains active but usually the severity of the lesions in these teeth is less than in the maxillary incisors. The mandibular incisors are usually not affected because the teat of the bottle is usually held above the tongue during sucking, so the lower incisors are protected by the tongue and also by the flow of saliva from the submandibular ducts [4]. The role of the innate infantile physiological tongue thrust pattern during deglutition is thought to be important in protecting the lower incisors [4].
In most cases of ECC, the first clinical sign is a band of dull white demineralization along the gingival line of the maxillary incisor teeth. As the lesion progresses, the white bands develop into cavities. This results in a brown or black collar around the necks of the incisors. In advanced cases, the lesions may become so severe that the crowns of the teeth are amputated leaving only decayed brownish-black root stumps (Figure 1). The commonly involved surfaces are the labial, palatal, mesial, distal of maxillary incisors and of the maxillary and mandibular canines. In the first and second primary molars, the occlusal surface is commonly affected [12]. According to Ripa [4], the reason for this unique distribution is related to three factors: 1) the chronology of tooth eruption; 2) the duration of the deleterious habit; and 3) the muscular pattern of infant sucking.
Fig 1. The clinical picture of ECC in early (A) and advanced stage (B) in a preschool child.
Prevalence of ECC The prevalence of ECC varies greatly in different studies. The prevalence worldwide has been reported to vary between 3% and 94%. This wide range may be due to several factors such as: 1) children studied; their age and the accessibility for examination; 2) socio-economic status; 3) ethnic and cultural factors and 4) criteria used for diagnosis.
The prevalence of ECC in one country usually cannot be compared with another [13]. Richardson et al reported that even results from one ethnic group cannot be extrapolated beyond that group, even within the same country [13]. In western societies, approximately 80% of caries is present in 20% of the population commonly in children from low socio-economic groups, certain immigrants, patients with learning difficulties and those with physical and medical disabilities. The dental survey of children aged one and half to four years in Great Britain [14] showed that the proportion of children affected increased with age: 4% of one and half to two and half year olds, 14% of two and half to three and half year olds and 30% of those aged three and half to four and half years had some experience of dental caries. In contrast, in the city of Abu Dhabi in the UAE, ECC in 2, 4 and 5 year olds is 35.5%, 85.7% and 93.8% respectively [6]. Hashim et al. (2006) in Ajman, UAE studied caries prevalence and severity of ECC in 5–6-year-old children. They reported high caries prevalence (76.1 %) and an average decayed, missing and filled surfaces (dmfs) score of 10.2 and that the Emirati (local) children had higher caries severity than other children [15]. Al-Hosani and Rugg-Gunn (1998) examined 5-year-old children in Alain city and reported a mean decayed, missing and filled teeth (dmft) score of 8.6 [6]. Recently, Kowash (2015) in a cross sectional study in the same city reported a higher mean dmft of 10.9 [16]. The aforementioned ECC prevalence results are clearly a cause of concern for this continuing problem in the UAE especially when comparing it with the internationally accepted definition of severe ECC (S-ECC).
Etiology of ECC The exact etiology of dental caries is still obscure. However, there is good scientific evidence to show that, for dental caries to occur, four main factors and some other minor or predisposing factors have to be present. Thus dental caries has a multifactorial etiology [17]. The four main factors are a susceptible host (teeth and saliva), a substrate (fermentable carbohydrate), micro-organisms (mainly streptococci and lactobacilli) and time. Predisposing factors include: feeding habits, oral hygiene practices, general health and nutritional status. Socio-economic factors (parental education and occupation, family income, number of siblings, parental attitude and knowledge of dental health) and demographic factors such as race, age, gender, soil and mater aspects are also contributing factors. These factors are often used as indicators to identify caries risk in children. The aetiology of ECC is indistinguishable from other coronal carious lesions in older children and adults. However, the lesion progresses rapidly and the cariogenic challenge overwhelms the protective mechanisms [18]. The etiology of the condition is a combination of frequent consumption of fermentable carbohydrates as drinks, especially at night time, with on-demand breast- or bottle-feeding because during sleep, salivary flow is greatly reduced. Other contributing factors include oral colonization by cariogenic bacteria (especially mutans streptococci) and poor oral hygiene [4]. In most cases of ECC, the etiology will be a combination of several of these factors.
There is a considerable debate in the literature regarding the effect of milk on teeth. Several studies considered it to be cariogenic under certain conditions [19, 20, 21]. Others have shown it to be anti-cariogenic [22, 23, 24]. Storey [25] reported that the reasons for this controversy are due to: 1) the difficulty of studying the effect of one item of food on dental health in human, 2) the difficulties of designing definitive nutrition experiments even in animals, 3) the different effects of food processing procedures on milk and 4) basic differences in the composition of milk of different species. The lactose (a disaccharide composed of glucose and galactose) content of human and bovine milk aids the implantation of cariogenic bacteria and produces enamel demineralization and caries when fed to animals [19]. The effects of milk on teeth depend upon the type of milk feeding, feeding practice and time of weaning.
It is difficult to identify which type of microorganisms are responsible for causing dental caries due to the complexity of plaque micro-organisms. However, mutans streptococci (MS) and lactobacilli (LB) are considered to be the most important cariogenic bacteria [26]. MS and LB can grow at an intracellular pH value lower than 6 (high aciduricity) and unlike most other bacteria, they can also produce lactic acid when exposed to high concentrations of sugars [27]. MS is responsible for initiation of carious lesion, whilst LB is responsible for the progression of the lesion and is the predominant microorganism of the cavitated carious lesion. The major source from which infants acquire cariogenic bacteria, especially MS, is the mother's saliva (vertical transmission). MS can also be acquired from other family members including child minders and nannies (horizontal transmission) [5]. Teeth provide a non shedding surface for colonization of MS and its counts are related to the number of erupted primary teeth [28]. However, recent studies have also shown that MS can colonize the mouth of pre-dentate infant [29, 30].
Consequences and complications of ECC
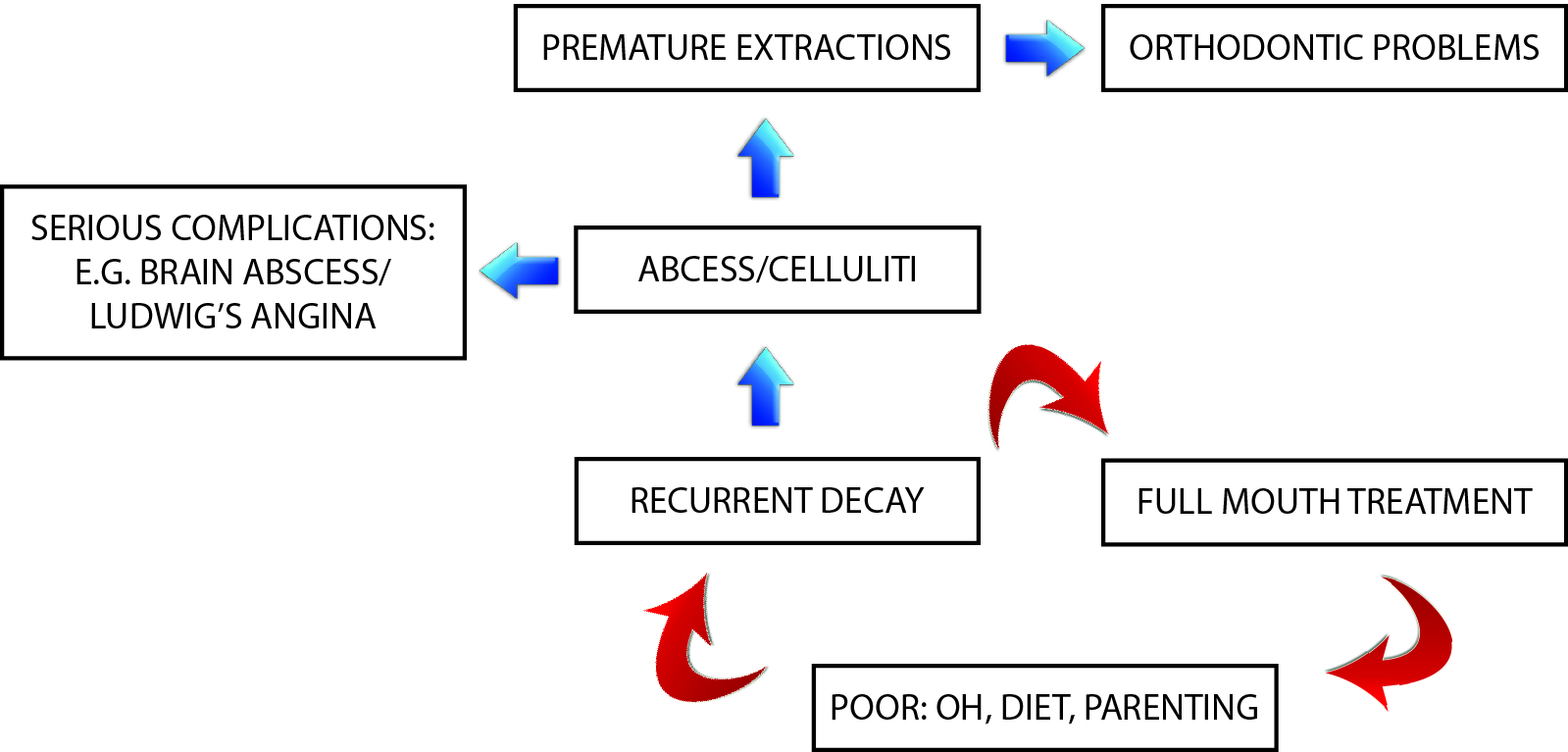
Depending on the severity and the extent of dental decay, ECC may lead to a significant impact on the child’s oral and general health. Deep untreated carious lesions lead to pain and discomfort, inability to properly chew food and the child may avoid eating because of pain which may lead to weight loss and failure to thrive [31]. In severe cases, pulpal necrosis in primary teeth may lead to a dental abscess formation which can cause pain and damage the developing permanent tooth. If there is a necessity for premature extraction, primary tooth loss may result in various orthodontic complications (Figure 2). Premature extraction of primary maxillary incisors may also lead to problems in speech, normal development of language and esthetic which may affect the personality and self- esteem of the child. Untreated ECC lesions may cause abscess, cellulitis and spread of infection, which may result in serious and fatal complications such as brain abscess and Ludwig’s angina (Figure 2). Management of ECC complications requires increased emergency room visits and hospitalization. The socio-economic consequences of ECC manifest in increased treatment costs and missing school time as well as time off from employment for parents [32, 33].
Management of ECC Prevention is the solution for the continuing problem of ECC. Despite following a high quality method for proper restoration of decayed teeth, recurrence of decay and its complications are very common in the absence of an adequate prevention program and follow up visits (Figure 2).
Fig 2. Vicious circle of treatment and re-treatment and its’ complications in the absence of an effective preventive strategy.
ECC is an infectious and transmissible disease but it is preventable. There are two main preventive programs: individual-based interventions and community-based interventions
Individual-based preventive programmes This approach is used for high-risk populations because it is simple and does not require much effort from the parent or caregiver. The disadvantages of an individual-based approach are twofold. Firstly, it requires identification of at-risk children and secondly, it can be costly as it requires professional or auxiliary personnel. Studies have used this approach by treating the mother by counselling, toothbrushing and use of fluoride to reduce the number of maternal micro-organisms transmitted to her child. Restoration of the mother’s open cavities and the use of anti-microbial agents can prevent or delay bacterial transmission to her infant [8].
The American Academy of Pediatric Dentistry (AAPD) [34] recommended dental health education program for parents with young children to improve their dental awareness and attitude toward dental health. The AAPD recommendations for the infant’s oral health include:
Establishment of a dental home: a dental consultation visit no later than one yr of age is recommended to educate parents and provide anticipatory guidance for prevention of dental diseases. The initial visit should include thorough medical (infant) and dental (parent and infant) histories, a thorough oral examination, performance of an age-appropriate tooth brushing demonstration and prophylaxis and fluoride varnish treatment if indicated.
Oral hygiene: oral hygiene measures should be implemented no later than the time of eruption of the first primary tooth. Twice-daily use of fluoridated toothpaste using a soft toothbrush of age-appropriate size. Parents should assess and supervise their preschool-age child tooth brushing. Infant’s newly erupted teeth may be cleaned using a cloth. Flossing of child’s teeth is recommended when adjacent tooth surfaces cannot be cleaned with a toothbrush.
Diet: Human breast milk has not been epidemiologically associated with caries. Frequent night time bottle feeding with milk is associated with but not consistently implicated in ECC. Breastfeeding greater than seven times daily after 12 months of age is associated with increased risk for ECC. Night time bottle feeding with juice, repeated use of a no-spill cup and frequent in between meal consumption of sugar-containing snacks or drinks (e.g. juice, formula, soda) increase the risk of caries. [35, 36]. Therefore, it is recommended that infants should not be put to sleep with a bottle after the primary tooth begins to erupt. Parents should be encouraged to have infants drink from a cup after one year of age. Repetitive consumption of any liquid containing fermentable carbohydrates from a bottle should be avoided.
Fluoride: Optimal exposure to fluoride is important to all dentate infants and children [37]. Decisions concerning the administration of fluoride are based on the unique needs of each patient [38]. The use of fluoride for the prevention and control of caries is documented to be both safe and effective [39].
Community-based preventive programmes To solve the problem of ECC there should be collaborative efforts of caregivers, health professionals, and the community [40, 41]. Weinstraub [41] believed that public health or community approaches are more necessary and effective than individualistic or behavioral approaches. Oral health professionals like dentists and hygienists should be trained for skills, as necessary, for developing community-based initiatives and dental programs. These skills would include maintaining knowledge of social beliefs, culture and practices and establishing and implementing dental prevention programs [42]. A successful long-term dental health education program through regular home visits to mothers with infants, commencing at or soon after the time of the eruption of the first deciduous teeth, was shown to be effective in preventing the occurrence of caries, improving oral hygiene and dental attendance of young children. An added benefit was that the mothers of the children also significantly improved their oral hygiene in terms of debris, gingivitis and calculus scores [9]. Young children are dependent on their parents or caregivers for their daily dietary and oral hygiene practices. Therefore, it is important that the dental health messages should focus on educating and changing the behavior of parents or caregivers. Moreover, the dental health messages should be practical by giving alternatives, for example substituting milk with water in baby bottles at night for those who find it difficult to stop night-time bottle feeding. They should also consider the socioeconomic status of the parents and be culturally sensitive [9]. The benefit-cost (B/C) and cost-effectiveness (C/E) of a long-term dental health education program to mothers with young children through repeated home visits were evaluated [43]. Comparisons were made for B/C and C/E with results from a clinical trial of a slow releasing fluoride device, community water fluoridation and a school based fissure sealant program. The results showed that dental health education programs for mothers of young children starting at 8 months of age gave better B/C and C/E ratios than other preventive programs.
Restorative treatment of ECC In recent years there has been a shift from the traditional (drill & fill) to a more conservative treatment modality (seal to heal) with better understanding of the caries process biology. Managing caries through minimally-invasive and low-cost treatment modality such as atraumatic restorative technique (ART) is important especially in developing countries. It helps in slowing caries progression and hence minimizing the child’s discomfort and preventing other decay complications. Studies have shown that, although caries causes demineralization of dental hard tissues and denaturation of collagen, the inner layer is minimally or even not infected by bacteria [44]. The inner part of decayed dentine contains a high concentration of minerals and can be rematerialized [45]. Management of ECC should take into consideration the biology of dental tissues, remineralisation process and other protective mechanisms. The goal should be to minimize lifelong caries experience while performing the least possible intervention consistent with level of risk (Table 1).
Findings
Caries Cavity
Status of carious lesion
Treatment modality
+ +
Manifested Caries
Arrest & restore (ART / Hall)
MS culture, counseling Restoration (not in every case) e.g. tooth-colored fillings, amalgam, SSC
+ -
Pre-manifested Caries
(white lesion)
Arrest process prior to cavitation e.g. fluoride varnish
- +
Post-manifested
(arrested) Caries
Maintain suppression of caries Restore lesion (ART, Hall)
- -
Inactive disease status
Anticipatory guidance
Table 1. Management of different stages of ECC
The type of restoration chosen depends on: the tooth to be restored, present and past caries history, child cooperation and medical history. For example a decayed primary molar in a special need child is best restored with a durable restoration like stainless steel crowns (SSC). A multi-surface decayed primary molar also should preferably be restored with SSC [46]. Grossly decayed maxillary incisors are best restored with either composite strip or zirconia crowns with or without pulp therapy (Figure 3). Depending on patient cooperation, the severity and number of decayed teeth and medical history, dental treatment of pediatric patient can be performed under behavior management and local analgesia, which is considered to be the best option in terms of cost, safety and acceptability to parents or caregivers. Other alternative options include oral or intravenous sedation and general anesthesia (GA). Full dental rehabilitation under GA (Figure 2) is preferred by many clinicians in uncooperative preschool children requiring comprehensive dental care or those with special needs.
All restorative techniques exhibit strengths and weaknesses for example:
Glass Ionomer Cement (GIC) is favorable for class I Cavities and in uncooperative children
Compomers shows best long-term performance. The cooperation has to be sufficient, at least during bonding and layering.
Resin composites after rubber dam application and correct technique – sensitive adhesion can reach the level of compomers.
In severely decayed teeth and after pulp therapy, preformed SSC should be the restoration of choice.
Fig 3. General anaesthesia full dental rehabilitation of a child with severe ECC: pre-treatment (A) and post- treatment (B).
Conclusion Early Childhood Caries (ECC) is a chronic, transmissible infectious disease affecting the primary teeth. The etiology of the condition is a combination of frequent consumption of fermentable carbohydrates as drinks, especially when a baby is sleeping, with on-demand breast- or bottle-feeding, oral colonization by cariogenic bacteria (especially mutans streptococci), poor oral hygiene and poor parenting. It is the most common chronic disease among children and is still considered a continuing oral health problem in developing countries and also in most developed countries. It can result in considerable suffering, pain, disfigurement, reduction of quality of life of affected children and frequently compromises their future dentitions. The treatment of ECC is very costly, time consuming and in most cases, requires full dental rehabilitation under general anesthesia by a pediatric dentist. ECC, however, is a preventable disease and the solution for this continuing problem can be achieved by educating parents of young children and pregnant mothers. It is important that the dental health messages should focus on educating and changing the behavior of parents or caregivers. Moreover, the dental health messages should be practical, consider the socioeconomic status of the parents and be culturally sensitive. The management of ECC should take in to consideration the biology of the caries process and protective mechanisms and to be effective, the restoration of active lesions should be monitored through regular follow up and long-tern preventive strategy.
Editorial note: The list of references is available from the publisher.
AL-AIN, UAE: According to the World Health Organization, 60 to 90 per cent of schoolchildren worldwide have dental cavities. Tooth decay, which can have a ...
On World Refugee Day, FDI World Dental Federation unveiled a pivotal policy brief titled Addressing Oral Health Needs in Refugees: Policy and Collaboration ...
Thousands of rural Kenyans have been helped out of poor oral health with treatment and preventive education by volunteers from dental charity Dentaid. ...
On the 24th of July with the representatives of Perio societies and clubs from five Arab countries (Egypt, Lebanon, KSA, UAE and Jordan the hosting ...
Every year on 20 March, the global dental community marks World Oral Health Day (WOHD) in the spirit of improving global oral health and overall well-being....
This year, the World Health Organization is bringing smiles to the forefront of global health with their gleaming new campaign: “A happy mouth is a ...
Dental Tribune Middle East had the pleasure of speaking with Dr Rafif Tayara, a distinguished consultant pediatric dentist with a passion for holistic care,...
HONG KONG: Autism spectrum disorder (ASD) is a global public health concern. Early identification and timely support for children with ASD can significantly...
AJMAN, UAE: Artificial intelligence (AI) is reshaping dental education by changing how students learn, educators teach and institutions prepare graduates ...
BAŞISKELE, Turkey: While traditional behaviour guidance techniques continue to play an essential role in managing anxiety and uncooperative behaviour in ...
JERUSALEM: Infertility is a major reproductive health concern worldwide, and a substantial proportion of cases have no clear explanation. Chronic oral ...

 International / International
International / International
 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس

 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Kubra Kundak, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Kubra Kundak, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CELive webinar
Cat EdneyRegister now1CELive webinar
 Dr. Allen Wong DDS, EdD, DABSCDRegister now1CE
Dr. Allen Wong DDS, EdD, DABSCDRegister now1CE












































To post a reply please login or register