Most dentists base their practice on an understanding of various risk factors thought to contribute to the common Dental Diseases. We have been taught that Dental Plaque (Biofilm) is universal in the development of caries and periodontal diseases, the former requiring the added ingredient of frequent sugar exposure and the latter, if it is to progress to significant bone loss, needing the presence of one or more of compounding factors such as Genetic Susceptibility, Smoking and Diabetes.
Accordingly, dental prevention has focused on effective regular plaque removal and a reduction in the frequency of sugar exposure and cigarette use, as well as the overeating/under-exercising combination which pre-disposes to type 2 Diabetes. Twice daily brushing with a fluoride containing toothpaste combined with interproximal cleaning as well as restriction of sugar exposures to mealtimes have been widely advocated as effective preventive measures, while twice yearly check-ups have been recommended to facilitate early detection and management of dental problems.
It is the purpose of this article to review the existing justifications for these commonly held beliefs and, where necessary, offer more evidence-based approaches to the effective reduction and ideally prevention of Dental Caries and Periodontal Diseases.
Measuring the Effectiveness of Preventive Measures Webster’s dictionary describes an OUTCOME as “Something that occurs as a result orconsequence of an action”. Most dental research uses Surrogate Outcomes to measure effectiveness of preventive and treatment interventions. These include a reduction in Plaque Index; less bleeding on probing (BOP), reduced percentages of bacterial pathogens and reductions in other easily measurable clinical and microbiological indices which assess hard or soft tissue as well as the quantity and quality of plaque. Ultimately patients are more interested in Real Outcomes that relate to their comfort and quality of life.
In medicine a new cancer drug may easily be assessed in its effectiveness of reducing blood white cell counts (a Surrogate Outcome) whereas 5 and 10 year survival rates when using the drug, compared to alternative treatments or a placebo are the Real Outcomes which are important to the patients. By definition they take many years to establish. In dentistry we are often presented with Surrogate Outcomes; for example, plaque removal using power verses manual toothbrushes, but seldom find True Outcomes such as comparative tooth loss or caries development when evaluating both. There are simple practical reasons for this. Studies using Surrogate Outcomes are relatively fast and cheap giving a sponsoring company results and a researcher a publication within a few months. Studies using Real Outcomes as measures are very costly; need larger sample sizes and take years to complete. Few companies and few researchers see corporate or academic benefits in participating. Yet these are the studies we need for long term effective prevention. Let’s look at what we have.
Dental Caries There are essentially 2 diseases to consider; Enamel Caries, most commonly seen in the first 30 years of life, and Root Caries, commonest in the last 30 years of life. From age 30 to 60 fresh carious lesions are uncommon except in extreme cases. Surrogate outcomes include plaque indices; percentage of decalcification and reduction in Lactinobacillus counts. For many years we have had a widely accepted real Outcome measure DMFT but because of the long-term nature of using this measure, commonly Surrogates are measured, with the implication that they can be extrapolated to Real Outcomes.
In a recent systematic review assessing the effect of Dental flossing on interproximal caries it was concluded that “…self-flossing has failed to show an effect” (1). In lay terms flossing does not work to prevent interproximal decay, although surrogate outcomes like plaque indices and bleeding on probing almost invariably improve.
If we cannot, honestly, advocate the use of floss to prevent caries, how about tooth brushing? Fortunately we have a longitudinal study with a 26 year follow-up that indicates that “…brushing at least once a day… 49% reduction in risk of tooth loss.” (2)
There is now also compelling evidence that power brushes are more effective than manual brushes in plaque removal and reduction of inflammation (3), however to date we have been unable to identify studies where these results can be extrapolated to real outcomes in the long term.
Traditionally the number of sugar exposures per day has been considered important in the initiation of careous lesions. Some studies support this; Ccahuana-Vásquez R.A et al in 2007 examined the “Effect of Frequency of Sucrose Exposure on Dental Biofilm Composition and Enamel Demineralization in the Presence ofFluoride” (4)
Ten volunteers living in a fluoridated area wore palatal appliances bearing human enamel slabs for 14 days. Slabs were exposed to 20% sucrose solution either 0 (control), 2, 4, 6, 8 or 10 x day and the volunteers used fluoride dentifrice 3 x day. Histologic and microbiological assessment led to the conclusion that “...the findings confirm that fluoride (3 times/day) can reduce enamel demineralization if sucrose consumption is not higher than 6 times/day.” (4)
How does this relate to the reality of general dental practice? It is a 14 DAY study with purely Surrogate Outcomes. No data on actual development of caries on patients’ teeth, no DMFT. It is a meaningless academic exercise leading to a publication after only 2 weeks of “clinical” research. Yet it is cited to confirm the conventional wisdom of number of exposures to sugar being more important.
By contrast Bernabé et al followed 1702 adults for over 11 years and concluded “... the amount of, but not the frequency of, sugars intake was significantly associated with DMFT throughout the follow-up period.” They go on to confirm that there is “... a linear dose-response relationship between sugars and caries, with amount of intake being more important than frequency of ingestion.” (5)
The length of this study is 11 years, not 14 days. The outcome (DMFT) is real not surrogate and the sample size is vast, compared to the 10 volunteers in Ccahuana-Vásquez study, and yet Cognitive Dissonance will lead many dentists to prefer the findings of Ccahuana-Vásquez since they reaffirm the prevailing conventional wisdom.
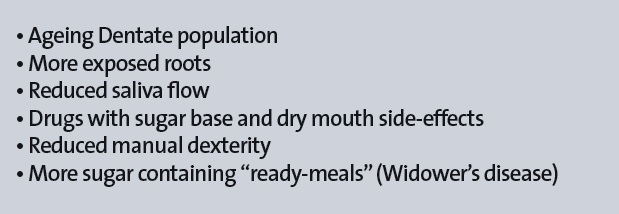
Root Caries is in fact a testament to the effectiveness of the dental profession in extending the life of teeth into old age. It is however a major challenge to a profession largely unfamiliar with its management. Factors contributing to this increasing problem are listed in Table 1.
Table 1: Factors contributing to the increase in root caries
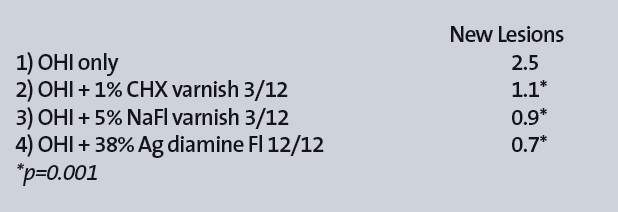
How can we minimize the development of root caries? A recent Randomised Controlled Trial (RCT) by Tan (6) investigated 306 generally healthy elders having at least 5 teeth with exposed sound root surfaces living in 21 residential homes. They were randomly allocated into one of four groups and followed for 3 years. A control group was given oral hygiene instruction and regular professional cleanings while 3 test groups had either 1% Chlorhexidine varnish or 5% Na Fluoride varnish applied every 3 months or 38% Ag Diamine Fluoride applied annually. The results are shown in Table 2.
Table 2: Root caries reduction using various topical agents (Tan et al 2010)
Clearly the dental and dental hygiene professions have an obligation to offer such active preventive measures to our ageing dentate population.
Periodontal Diseases While Bacterial Plaque is a necessary ingredient in the development of periodontal diseases, the fanaticism with which the Dental and Dental Hygiene professions have focused on “plaque control” has taken attention away from the important role of other risk factors. It is beyond the scope of this article to discuss genetic predisposition to periodontal diseases, and at present this appears to be a non-correctible factor largely managed by extra vigilance. We should however be aware of the relative importance of Bacterial Plaque, Smoking and type 2 Diabetes as major, potentially manageable, periodontal risk factors.
Bacterial Plaque In a systematic review examining the efficacy of dental floss in addition to a toothbrush on plaque and parameters of gingival inflammation, Berchier et al concluded that the evidence reviewed “….did not show a benefit for floss on plaque and clinical parameters of gingivitis” (7)
On the other hand, several studies have shown that thorough tooth brushing even once a day effectively controls these same surrogate measures. (8) (9)
In an 8 year study of treated periodontitis patients, Ramfjord et al 1982 (10) found that the quartile with the worst OH did just as well as the quartile with the best OH PROVIDED they had a one hour hygiene maintenance visit every 3 months. They measured attachment levels, a true outcome. One should bear in mind however that even the worst quartile had a reasonably low plaque index compared to baseline.
In assessing the importance of periodontal patient compliance (attendance) with a recall regimen, a Systematic Review of 710 articles, of which 8 were selected with a minimum 5 year follow-up concluded that the Erratic Compliance group have almost double risk of tooth loss compared to regular compliance group (a TRUE OUTCOME) (11).
While there may be many situations in the periodontal patient where flossing and other interproximal cleaning methods may assist in preventing or delaying disease progression, it is now clear that, as a universally recommended method for prevention of the commoner dental diseases, routine use of dental floss offers little if any benefit. The profession should focus on effective brushing and regular attendance.
Smoking We have known for over 20 years of the association between smoking and progression of Periodontal diseases. Smoking significantly increased the risk of tooth loss due to periodontal disease (Odds ratios (OR) 2.5 to 6.6). When corrected for other variables, smoking significantly increased the risk of increased attachment loss compared to matched non-smokers (OR 2.4 to 9.2) (12)
A longitudinal study of 349 patients followed for 10 years found that smokers lost almost twice as much bone as non-smokers over this period, while a smoker who quit had slower bone loss than the continuing smoker (13).
In a later study Hyman and Reid (2003) assessed loss of attachment – another True Outcome – differentiating between younger and older patients and found an OR of 18.6 of Loss of attachment >3mm in Smokers age 20 to 49. Not surprisingly a Loss of attachment >4mm in Smokers age over 50 had an even greater OR of 25.6 (14).
Rather than try to use multiple figures such as the above, I feel it is reasonably to advise smoking patients that continuing smokers progressively increase the risk of tooth loss, and that by the time they have smoked 20 cigarettes a day for 20 years (20 pack/years) they are around 600% more likely to lose teeth due to periodontal disease (OR 6).
Smoking cessation counseling should thus be as fundamental to dental prevention as is oral hygiene instruction.
Diabetes Preshaw et al in 2012 (15) described both a clear relationship between degree of hyperglycaemia and severity of periodontitis as well as describing a risk of cardiorenal mortality (ischaemic heart disease and diabetic nephropathy combined) which is three times higher in diabetics with severe periodontitis than in diabetics without severe periodontitis. This 2 way relationship between these 2 major diseases mandates not only effective glycemic control in order to achieve the best outcomes of periodontal therapy, but also effective periodontal management to reduce the risk of the severe complications of diabetes.
In a systematic review and meta-analysis Engebretson and Kocher (2013) (16) found a mean treatment effect of a reduction of HbA1c of -0.36% after periodontal treatment in type 2 diabetics. This is considered equivalent to the type 2 diabetic needing one less drug for glycemic control.
In a recent controlled study in pre-diabetics, thorough non-surgical periodontal treatment reduced the HbA1C levels of the participants by over 1%. (17)
According to Diabetes UK, if such a reduction could be sustained in Diabetic patients in might result in a baindiabetic being 19% less likely to suffer cataracts, 16% less likely to suffer heart failure and 43% less likely to suffer amputation or death due to peripheral vascular disease. Clearly these are enormous potential health benefits.
Discussion It seems apparent that many of our traditional approaches to prevention, while clearly well intentioned, have a weak evidence base. It is challenging for any health care professional to be asked to question the veracity and benefits of a long-used set of preventive recommendations and there will inevitably be a temptation to lapse into Cognitive Dissonance and possibly even denial. It is however our Duty of Care to offer all patients the most current evidence-based advice for the prevention and management of dental diseases.
It is beyond the scope of this article to address the relationship of the various risk factors to Peri-Implant diseases and implant failure. In view of the rapid increase in the use of dental implants and the self-evident truth that the vast majority of implant patients lost teeth due to Caries or Periodontal Disease, it is equally important that dental health care professionals appreciate the relative importance of the risk factors outlined above on Peri-implant diseases. In a very recent extensive retrospective study Derks et al (18) identify moderate to severe peri-implantitis in 14.5% of implant patients examined, and report on the Odds Ratios of the various influencing factors. In a commentary on this study Tarnow (19) points out that even a modest incidence of 10% of patients with Peri-implantitis equates to 100000 new cases of Peri-implantis every year based on current numbers of implants being placed. It might be appropriate to consider this in a future review article.
Conclusions Our understanding of the relative importance of the various major risk factors for Caries and Periodontal diseases should be evidence based and current. At present it is reasonable to conclude the following:
Recent research has indicated that the total amount of sugar consumption is more important than the number of sugar exposures per day in the development of coronal caries.
There is little to support the use of dental floss as a preventive measure for dental caries or gingivitis.
Effective toothbrushing, using a fluoride toothpaste and a power brush, is by far the most effective preventive measure to minimize dental caries and periodontal diseases.
To minimize the incidence of root caries in the elderly oral hygiene must be supplemented with periodic application of a fluoride or Chlorhexidine preparation.
While oral hygiene is important in controlling Periodontitis in the susceptible patient, compliance with a comprehensive Supportive Periodontal Maintenance Recall regimen is likely even more critical in preventing progression and tooth loss due to Periodontitis.
To achieve the best outcomes in periodontally susceptible patients who smoke, smoking cessation programmes must accompany traditional “Hygiene” phase therapy.
To achieve the best outcomes in diabetic patients with Periodontitis the dental professional must work closely with the medical clinician responsible for diabetes care. Improvements in one disease are likely to be complimented by improvements in the other.
When assessing the relevance of clinical research more credence should be given to longer term studies measuring REAL outcomes than shorter term studies which use SURROGATE outcomes.
Periodontal diseases have, for a half of a century, been known to be initiated by the accumulation of bacterial plaque (R). It has however been increasingly...
CAPE TOWN, South Africa: Although a number of studies have already suggested a link between periodontal disease and adverse pregnancy outcomes, the matter ...
Heart attack is the leading cause and diabetes is the sixth-leading cause of death in the United States.1 What goes relatively unnoticed, however, are their...
ŌTSU, Japan: The links between diabetes, obesity and periodontal disease are well established; however, most studies on their associations have had sample ...
NEW YORK, US: Studies have repeatedly shown that oral bacteria can contribute to periodontal disease. Now, researchers have sought to examine whether there ...
Presented here is a guided biofilm therapy case with the aim of achieving improved periodontal health in a nervous patient. Treatment was carried out over a...
The combination of Chlorhexidine Digluconate (CHX), professional reference for plaque control and Cetylpyridinium Chloride (CPC), included in GUM Paroex ...
OMDURMAN, Sudan: An international team of researchers has found new evidence that prehistoric ancestors had a detailed understanding of plants long before ...
JOHANNESBURG, South Africa: In 2018, South Africa introduced a tax on sugar-sweetened beverages (SSBs) based on their respective levels of sugar content ...
KUWAIT CITY, Kuwait: The majority of sugar-free chewing gums containing xylitol that are sold in the Cooperation Council for the Arab States of the Gulf ...
Education
Live webinar Tue. 4 August 2026 4:00 am UAE (Dubai)
AJMAN, UAE: Artificial intelligence (AI) is reshaping dental education by changing how students learn, educators teach and institutions prepare graduates ...
BAŞISKELE, Turkey: While traditional behaviour guidance techniques continue to play an essential role in managing anxiety and uncooperative behaviour in ...
JERUSALEM: Infertility is a major reproductive health concern worldwide, and a substantial proportion of cases have no clear explanation. Chronic oral ...

 International / International
International / International
 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس

 Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CE
Cat EdneyRegister now1CE









































To post a reply please login or register