Managing the carious primary molar in children using the “Hall Technique” is a controversial but acceptable novel method. Restoring all eight carious primary molars in a single child by using this technique, however, has not been reported by those who advocate its use. We report a case in which the Hall technique was employed to maximum capacity, out with normal practice, to restore all Es and Ds in a three year old child (hence the name All Hall).
Follow up showed no clinical or radiographic complications. This negated the need for unnecessary invasive treatment under local anaesthesia or general anaesthesia. In this article the concept of “All Hall” is introduced as a convenient and cost effective tool in the management of all carious primary molars in a single child. It is relevant to GDPs, working in busy practice environments, keen to avoid child LA treatment or GA referrals. The reader should understand that it is possible to restore eight carious primary molars in one child using the HT.
Introduction
The carious primary molar is a clinical problem reported, in the paediatric dental literature1, to have several solutions. These management options range, historically starting from conventional surgical treatment involving the excision of caries (under local anaesthesia) and restoring the tooth and ending simply by managing the plaque’s biological environment employing minimal interventional techniques2.
One example of the latter is the “Hall Technique or HT”3,4 which entails entombing the carious lesion by sealing it from the oral environment using a preformed metal crown (the stainless steel crown or SSC). The HT is usually prescribed to manage carious primary molars according to clear selection criteria and was developed in the UK as a child friendly treatment modality5.
Although conventional restoration of all primary molars using SSCs has been the norm for many years, this had not been the same when using the HT. The operating manual of the HT stated that “Hall crowns are not a universal answer to managing all carious primary molars and the Hall Technique does not suit every carious primary molar in that child”3. Therefore it became current acceptable clinical practice, by those who advocate the use of the HT, not to restore all the primary molars in one child using this technique. In other words, restoring all carious Ds and Es in one single child, using the HT was inadvisable. The reasoning behind this had not been clarified, but it may possibly be due to perceived concerns about the occlusion. The effect of the HT on the occlusion had been previously studied6,7. The occlusion tended to suffer opening of the bite by 1.5mm on average, which later resolved due to possible dento-alveolar compensation6 or intrusion7 of the crowned tooth. The effect was studied when one or two crowns were placed, however no study had shown the effect of restoring all Es and Ds in one child, on the occlusion.
We report a case whereas the HT was deployed to maximum capacity, contrary to the usual clinical doctrine, to restore all eight primary molars in one child. There were no known complications and the occlusion was deemed satisfactory. This case had been labeled the “All Hall” case.
Case report
A fit and healthy three year old boy (MF) attended with his father to the Department of Paediatric Dentistry at Hamdan Bin Mohammed College of Dental Medicine (HBMCDM) in Dubai Healthcare City, Dubai (UAE). The father was concerned about ‘holes in his son’s teeth’. The father reported that MF suffered no pain whatsoever. After clinical and radiographic examination, MF was found to have multiple asymptomatic carious primary molar and incisor teeth fitting with the diagnosis of Severe Early Childhood Caries (S-ECC). Interestingly, MF’s eight carious primary molars (55, 54, 64, 65, 75, 74, 84 & 85) were free from symptoms of pain, and clinical and radiographic signs of pulpal pathosis. See Figures 1 (a, b, c, d & e) for clinical features, and Figures 2 (a & b) for radiographic findings.
He also had initial caries on 53, 52, 51, 61, 62 & 63. There was no known trauma history. His initial cooperation was categorized as “pre-cooperative”. MF’s behavioural scale was assessed to be negative initially but improved dramatically to positive behavior as treatment progressed. Treatment options for the carious primary molars that were discussed and explored with MF’s father were; prevention only, conventional restorative treatment using local anaesthesia (LA), the “Hall Technique” with no LA (and restorations of the upper primary incisors) or full mouth rehabilitation under general anaesthesia (GA). MF’s father was keen for his son to receive dental treatment in the dental chair rather than under GA due to many reasons including financial constraints (children’s dental GA is not routinely provided by a free public service -available to everyone- in the UAE as it is in the UK for example). After sufficient consideration, the father consented for the HT as the child’s cooperation for LA was not forthcoming and he was adamant about avoiding GA.
Figures 1 (a, b, c, d & e) are showing typical dental caries in a 3 year old. He had no symptoms whatsoever. In Figures 1 b & d an orthodontic separator can be seen fitted distally to 64.
Figures 2 (a & b): Bitewing radiographs showing caries on all Ds and Es. There were clear bands of dentine between the carious lesions and the pulp. There were no radiographic signs of interradicular pathology. Although the furcation areas of upper Es were not visible, no further xrays were justified as the upper Es had shallow radiographic lesions.
Figures 3 (a, b, c, d & e): Immediate post- treatment completion images. All Es and Ds were restored using the HT. Notice the good gingival status. Using the primary canines as a guide, opening of the bite is noted in Figures 3 (d & e). 51 became discoloured with no sinus present. No known trauma. We opted to manage 51 conservatively as x-ray showed no pathology. The patient by this time had no experience of LA, avoided GA and was gradually becoming cooperative.
Figures 4 (a, b, c, d & e): 9 months post- treatment. The patient had no complaints. The occlusion had equilibrated (note primary canines in Figures 4 b & c and compare to Figure 3 a, d & e). All Es and Ds remained asymptomatic. Good gingival health and oral hygiene were noted. As his cooperation improved plans are in place to monitor 51 with a view to carry out pulp therapy in addition to restoring upper anteriors with composite strip crowns.
Treatment
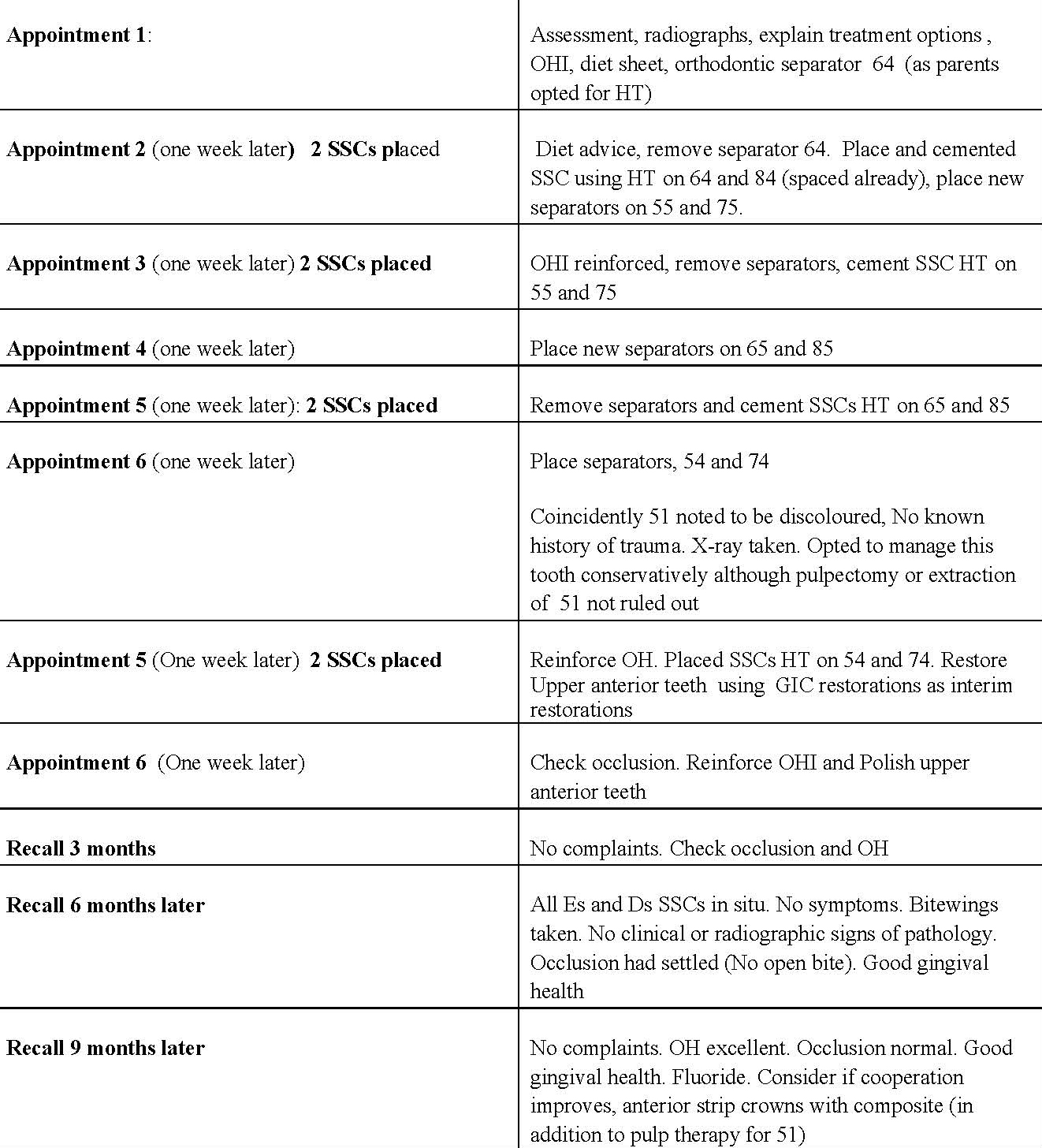
A treatment plan was arranged on our postgraduate clinic (See Table 1). An extensive preventive programme was instigated to improve MF’s very poor oral hygiene in addition to diet assessment, analysis and advice.
Over a period of two months and following the HT protocol3, the child had all his eight primary molars fitted with SSCs and cemented with GIC. No LA was used. The molars were fitted with elasticated orthodontic separators in order to create space to prepare the teeth to receive the SSC a week later. Two molars were treated per appointment (see Table 2).
Table 1. Treatment plan
Table 2. Sequence of appointments
As per the standard Hall manual3, the following principles were adhered to during treatment:
1) Compliance with the indications and contra indications and selection criteria for the HT5. Assurance of the absence of any symptoms or signs of pulpal pathosis or sepsis (clinical or radiographic assessments).
2) Blue elasticated orthodontic separators were used and left in situ for one week (see Figure 1b & d) to create interdental spaces where required.
3) Two SSCs placed in a single appointment were never:
a. In the same arch adjacent to each other (i.e. never in the same quadrant)
b. On the same side in opposing arches
4) When two crowns were placed in a single appointment they were diagonally in opposing arches (for example 64 and 84).
5) Appointments were at least one to two weeks apart to allow the occlusion to settle. The appointments were short; no longer than 15-20 minutes.
The SSCs crowns were placed as per the schedule in Table 2. The patient also had simple restorations placed (with no LA) on his upper anterior primary incisors and canines, using simple excavation and GIC with a view to eventually receiving composite strip crowns. Figures 3 (a, b, c, d & e) show the mouth immediately after completion of treatment. The bite appeared open and was initially raised by approximately 1-1.5 mm.
The patient was followed up three, six and ninth months later. He, nor his parents, had any complaints whatsoever. There were no issues with the occlusion, symptoms or signs of pulpal pathosis or sepsis affecting the molars. The bite had completely recovered. See Figures 4 (a, b, c, d & e). The parents’ satisfaction in reaching a positive outcome, without resorting to the use of GA, was very high. Post op radiographs (Figures 5 a & b) showed satisfactory clown placement and no recurrent caries.
Long term treatment plan:
1. Continue follow up at 3 months intervals of all Es and Ds clinically.
2. Close monitoring of tooth 51 for any sign of infection. Pulpectomy or extract if symptoms.
3. Bitewing radiographs every 6 months to monitor all Es and Ds. Interval to increase if caries risk status changed.
4. Restore remaining upper anterior teeth with composite strip crowns once cooperation allows.
5. Reinforce preventive measures (oral hygiene, diet), professional topical fluoride varnish application 4 times/year.
Discussion
In 2007 a new technique took the paediatric dentistry world by suprise4. It recommended a simple way in managing early enamel and dentinal decay in the primary molar using a SSC; it was named the Hall technique (HT) after UK based Scottish dentist Dr. Norna Hall started using this method5. The HT involved no local anaesthesia, no rubber dam, no drilling and took place in a child friendly play manner. No dental caries removal took place at all. The HT relied on sealing caries in situ cutting off its supply of sugary substrate, therefore changing the lesion’s bacterial plaque and resulting in the arresting of the caries process in the tooth1. The HT was confirmed as a mainstream modality in treating carious primary molars1,2 after a prospective split mouth randomized control study was conducted showing very high success rates of the HT after two4 and five years8. There were mixed international reactions to the development to the HT in paediatric dentistry circles with many advocating such a treatment method9,10,11 while others opposed it completely12,13,14. At the time of writing this article, this healthy debate was still in progress15. It is important to note that there is no disagreement about the fact that SSCs are the restorative materials of choice in multi-surface caries affecting primary molars16. The disagreement lies in the method used to apply them.
This report showcased treatment that may be of interest to general dental practitioners (GDPs) and specialists in paediatric dentistry alike. It highlighted simple non- invasive treatment that eliminated the need for treatment under LA and avoided a dental GA in a very young child. A situation many face in practice on a daily basis.
This case had been a great challenge due to important factors which were; the patient’s young age, anxiety, the number of molars involved, pre-cooperation, the limited financial capacity of the parents to afford general anaesthesia and the scepticism that other dentists15 had of the HT. However, the parent’s dedication to attend to multiple appointments, motivation and great support to their child made it successful. Modelling techniques had worked successfully to reduce MF’s dental anxiety, where he observed and learned appropriate behaviour from his parents and sister. Separation anxiety is very common at this age and having the parent or his sister around was helpful. MF had a high risk dental caries status, so his primary molars were treated using SSCs, although other options such as complete caries removal and composite restorations, partial caries removal or even non restorative caries treatment (NRCT)1 were possible.
MF was a good candidate for the HT, as his moars were carious, asymptomatic, had no signs of irreversible pulpitis or sepsis, no clinical or radiographic signs of pulpal involvement or inter-radicular pathology and had a good amount of tooth structure for crown retention. In other words, the molar lesions were “captured” before they became pulpally involved. The HT was effective as it sealed the caries under the crown without local anaesthesia, tooth preparation or caries removal. Priority was given to tooth 84 as it had the deepest lesion compared to the rest.
MF accepted the minute occlusal changes after cementation of each HT crown. The occlusion clinically appeared to have re-established itself in a very short time (see Figures 3 and 4 using the primary canines as indices) and this was always checked before proceeding with the next phase.
Managing the upper anterior cavities with permanent restorations would have been impossible in this case due to the child’s lack of cooperation. Therefore, temporization of open cavities with GIC was a straightforward way to introduce the child to dental procedures. It was also advantageous in terms of preventing the progression of caries, reducing the chance of sepsis and pain, reducing the oral load of plaque and a good source for fluoride. Composite strip crowns will be considered as an alternative if cooperation allowed. Coincidently the patient’s 51 became discoloured, albeit asymptomatic. Although no history of trauma was elicited in this case, it was assumed to be the case. Persistent dark discolouration in the patient’s 51 may be associated with pulp necrosis. Since the tooth is asymptomatic clinically and in the absence of radiographic pathological signs (Figure 5 c), it was decided to keep under close review. Parents were aware that this tooth may require future treatment; a pulpectomy or extraction.
As for the Es and Ds, the patient was followed up for ninth months after treatment was completed. He remained clinically free of symptoms and became a patient who enjoyed attending our clinic. They will remain under observation in the long term. Plans are in place to manage his upper anterior teeth as outlined above.
Conclusion
This case is an “All Hall” case where maximum capacity of the HT was used in one single child. The HT is one tool in the toolkit available to dentists in the fight against dental caries11.
Although well designed trials are in place to support the HT, this case highlights that restoring eight carious primary molars in one child, with no short to medium term complications, is achievable using the HT. The lesions need to be “caught” prior to any pulpal involvement.
It may be of interest to GDPs and primary care dentists, rather than specialists in paediatric dentistry, who deal with the majority of child dental patients. The HT is a suitable modality for the GDP environment, hence this case report.
References
1) Kidd, E. Should deciduous teeth be restored? Reflections of a cariologist. Dent Update 2012; 39: 159–166.
2) Scottish Dental Clinical Effectivness Programme. Prevention and Management of Dental Caries in Children Dental Clinical Guidance. SDCEP Manual. http://www.sdcep.org.uk/wp-content/uploads/2013/03/SDCEP_PM_Dental_Caries_Full_Guidance1.pdf
3) Evans, D & Innes N. The Hall Technique. A Minimum intervention, child centred approach in managing the carious primary molar. A user manual. Free downloadable online manual. http://dentistry.dundee.ac.uk/sites/dentistry.dundee.ac.uk/files/3M_93C%20HallTechGuide2191110.pdf
4) Innes NP, Evans DJP and Stirrups DR. The Hall Technique; a randomized controlled clinical trial of a novel method of managing carious primary molars in general dental practice: acceptability of the technique and outcomes at 23 months. BMC Oral Health 2007, 7:18. Available online at http://www.biomedcentral.com/1472-6831/7/18
5) Innes NP, Evans DJP, Hall N. The Hall Technique for Managing Carious Primary Molars. Dent Update 2009; 36: 472–478.
6) van der Zee V, van Amerongen WE. Influence of preformed metal crowns (Hall Technique) on the occlusal vertical dimension in the primary dentition. Eur Arch Paediatr Dent 2010; 11: 225–227.
7) So D, Evans, D, Borrie F, Roughley M, Lamont T, Keightley A, Gardner A, Hussein I, De Souza N, Blain K, Innes NP. Measurement of occlusal equilibration following Hall crown placement; pilot study. Presentation to the International Association of Dental Research (IADR), Boston, USA, March 2015 (Abstract). J Dent Res, 2015; 94: A.
8) Innes NP, Evans DJP and Stirrups DR. Sealing caries in primary molars: randomized control trial, 5-year results. J Dent Res 2011; 90:1405-1410.
9) Santamaria R, Innes N, Machiulskiene V, Evans D, Alkilzy M, Splieth C. Acceptability of different caries management methods for primary molars in a RCT. Int J Paed Dent 2015; 25:9-17
10) Ludwig KH, Fontana M, Vinson LA, Platt JP, Dean JD. The success of stainless steel crowns placed with the Hall technique: A retrospective study. JADA 2014; 145:1248-1253.
11) Hussein, I. The Hall technique: The novel method in restoring the carious primary molar that is challenging old concepts. A new tool in the general dentist’s toolbox? Dental Tribune 2015; 4: 18-20.
12) Hashim Nainar SM. Success of Hall crown questioned. Pediatr Dent 2012; 34:103
13) Yalgnkaya Erdemci Z, Burgak Cehreli S, and Ebru Tirali R. Hall versus conventional stainless steel crown techniques: in vitro investigation of marginal fit and microleakage using three different luting agents. Pediatr Dent 2014; 36: 286-90
14) Seale, NS & Randall, R. The use of stainless steel crowns: A systematic literature review. Pediatr Dent, 2015; 37: 147-162
15) Croll TP, Killian CM, Simonsen RJ. The Hall technique: serious questions remain. Inside Dentistry 2015; 6: 30-32.
16) Kindelan SA, Day P, Nichol, R, Willmott, N & Fayle SA. UK national clinical guidelines in paediatric dentistry: stainless steel preformed crowns for primary molars. Int J Paed Dent 2008; 18(Suppl. 1): 20–28.
Primary molar dental caries in childhood is a disease of epidemic proportions that affects all modern societies. Despite a World Health Organization (WHO) ...
Implant prosthetics and dental prosthetics differ considerably, with the absence of periodontal ligament in the implant/prosthesis complex. This situation ...
The COMBI touch combines ultrasound and air-polishing in one unit to provide a complete prophylaxis treatment from removal of supra-gingival and subgingival...
Based on our long-term bonding expertise, we developed GLUMA Bond Universal – a universal bonding answering to all your bonding needs. It is a reliable ...
As CEO of 3DVision, a provider of premium digital dentistry solutions and education, Dr Rami Gamil has become a driving force in advancing digital workflows...
Dr Yasser Khabbaz is a consultant periodontist and implantologist at Ambulatory Healthcare Services in Abu Dhabi and runs a practice limited to periodontics...
Align Technology, a leading global medical device company that designs, manufactures, and sells the Invisalign system of clear aligners, iTero intraoral ...
AJMAN, UAE: Artificial intelligence (AI) is reshaping dental education by changing how students learn, educators teach and institutions prepare graduates ...
BAŞISKELE, Turkey: While traditional behaviour guidance techniques continue to play an essential role in managing anxiety and uncooperative behaviour in ...
JERUSALEM: Infertility is a major reproductive health concern worldwide, and a substantial proportion of cases have no clear explanation. Chronic oral ...

 International / International
International / International
 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس

 Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CE
Cat EdneyRegister now1CE




















 are showing typical dental caries in a 3 year old. He had no symptoms whatsoever. In Figures 1 b & d an orthodontic separator can be seen fitted distally to 64.")
: Bitewing radiographs showing caries on all Ds and Es. There were clear bands of dentine between the carious lesions and the pulp. There were no radiographic signs of interradicular pathology. Although the furcation areas of upper Es were not visible, no further xrays were justified as the upper Es had shallow radiographic lesions.")
: Immediate post- treatment completion images. All Es and Ds were restored using the HT. Notice the good gingival status. Using the primary canines as a guide, opening of the bite is noted in Figures 3 (d & e). 51 became discoloured with no sinus present. No known trauma. We opted to manage 51 conservatively as x-ray showed no pathology. The patient by this time had no experience of LA, avoided GA and was gradually becoming cooperative.")
: 9 months post- treatment. The patient had no complaints. The occlusion had equilibrated (note primary canines in Figures 4 b & c and compare to Figure 3 a, d & e). All Es and Ds remained asymptomatic. Good gingival health and oral hygiene were noted. As his cooperation improved plans are in place to monitor 51 with a view to carry out pulp therapy in addition to restoring upper anteriors with composite strip crowns.")
 are showing typical dental caries in a 3 year old. He had no symptoms whatsoever. In Figures 1 b & d an orthodontic separator can be seen fitted distally to 64.")
: Bitewing radiographs showing caries on all Ds and Es. There were clear bands of dentine between the carious lesions and the pulp. There were no radiographic signs of interradicular pathology. Although the furcation areas of upper Es were not visible, no further xrays were justified as the upper Es had shallow radiographic lesions.")
: Immediate post- treatment completion images. All Es and Ds were restored using the HT. Notice the good gingival status. Using the primary canines as a guide, opening of the bite is noted in Figures 3 (d & e). 51 became discoloured with no sinus present. No known trauma. We opted to manage 51 conservatively as x-ray showed no pathology. The patient by this time had no experience of LA, avoided GA and was gradually becoming cooperative.")
: 9 months post- treatment. The patient had no complaints. The occlusion had equilibrated (note primary canines in Figures 4 b & c and compare to Figure 3 a, d & e). All Es and Ds remained asymptomatic. Good gingival health and oral hygiene were noted. As his cooperation improved plans are in place to monitor 51 with a view to carry out pulp therapy in addition to restoring upper anteriors with composite strip crowns.")

























To post a reply please login or register