Molar incisor hypomineralisation (MIH) is a relatively common dental defect that appears in first permanent molars and incisors and varies in clinical severity. The specific etiological factors remain unclear. Inappropriate diagnosis can result in mismanagement of the condition and results in early loss of first permanent molars (FPM) in particular. Therefore, the early identification of such condition will allow early intervention including monitoring and preventive interventions that might help in remineralisation of the hypomineralised tooth structure. These preventive measures can be instituted as soon as affected surfaces are accessible.
Clinical relevance statement
Failure of early diagnosis and dental management in cases of Molar Incisor Hypomineralisation (MIH) leads to rapid development of dental caries, increased pulpal inflammation and continuous enamel as well as restoration breakdown.
Objective statement
The reader should understand the Molar Incisor Hypomineralisation (MIH) condition and the availability of different management options of this condition.
Introduction
Molar Incisor hypomineralisation (MIH) is a developmentally derived dental defect that involves hypomineralisation of 1 to 4 first permanent molars (FPM), frequently associated with similarly affected permanent incisors. The pattern of enamel defects consists of asymmetric, well-demarcated defects affecting the enamel of the FPMs and is associated with similar defects in permanent incisors and canines tips. (1)
~ Prevalence
Available modern clinical prevalence data for MIH, mostly from Northern Europe, ranges from 3.6% to 25% and seems to differ between countries and birth cohorts. (2)
~ An etiology
An etiology of this condition is poorly understood, with many associated factors (including environmental changes, breast feeding, respiratory diseases, oxygen shortage of ameloblasts and high fever diseases) but few proven causative agents. (3)
~ Clinical Features
Fairly large demarcated opacities, whitish-yellow or yellowish-brown in colour that may or may not be associated with post eruptive enamel breakdown.Hypomineralised enamel can be soft, porous and look like discoloured chalk or Old Dutch cheese. Subsurface porosity leads to breakdown after eruption, especially under occlusal forces, resulting in exposed dentine and sensitivity. (4)
~ Management
Permanent molars affected by hypomineralisation are prone to rapid development of dental caries and repeated breakdown of restorations.Therefore, careful planning is required, taking into account patient’s age (behaviour management issues), degree of crowding and co-operation. Sensitivity of affected teeth plays a major role in difficulty of achieving anaesthesia and thus behavioural issues.
- Preventive
• Diet advice • Higher fluoride toothpaste (at least 1450ppm F)
• Topical fluoride varnish
• Casein phopshpeptide-amorphous calcium phosphate (CPP-ACP)
- Restorative:
• A small lesion can be treated with localized composite, where the enamel is soft, or fissure sealants, where the hardness of the enamel appears no different from the unaffected enamel.
• GIC is recommended as dentine replacement or as an interim restoration due the ease of placement, fluoride release and chemical bonding.
• For extensive lesions with post-eruptive breakdown especially if the cusps are involved, preformed stainless steel crowns (SSCs) are preferred as an effective medium-term restoration. SSCs can preserve the FPM until cast restorations are feasible. (5)(6)
- To save the tooth or not?
• The first decision in the management of the MIH FPM is whether the tooth should be saved or not. The decision to extract or restore will depend upon a number of different factors, some of these being the degree/extent of hypomineralisation, post-eruptive breakdown, sensitivity, age and co-operation of the patient, any developmentally absent teeth. Consultation with an orthodontist is advised.
According to the Royal College of Surgeons of England Guidelines for the Extraction of First Permanent Molars in Children, the ideal timing of first permanent molar extraction is between 8-10 years of age after the eruption of the lateral incisors but before the eruption of the second permanent molars and second premolars. Traditionally, for the most optimum mesial movement of the second permanent molar to occupy the place of the extracted FPM and produce the best occlusal position, t it has been suggested that the second permanent molar is demonstrating radiographic evidence of calcification in the root bifurcation. (7)
Case report
A ten-year-old patient (S.S) with no significant medical history or allergies presented to the Department of Paediatric Dentistry at Hamdan Bin Mohammed College of Dental Medicine (HBMCDM) in Dubai Healthcare City, Dubai (UAE). Complaining of slight pain due to a dislodged filling in her upper left region. Presently the tooth is asymptomatic. The pain is described as intermittent during the day, lasts for a while (hour or less), does not stop her playing or affect her sleep.
Detailed history was taken from the father. The father reported that (S.S) had a significant number of upper respiratory tract infections and tonsillitis during early years of life.Clinical and radiographic examination of (S.S) revealed yellowish discoloration of the enamel on the occlusal surfaces of 16 and 26. 26 presented with a dislodged filling, 36 and 46 had big composite fillings. The presentation of the FPM is consistent with the diagnosis of molar incisor hypomineralisation (MIH) without incisor involvement. The oral soft tissue appeared healthy with fair oral hygiene, microdontia of upper lateral incisors (peg shaped), with Stained fissures of lower primary molars.
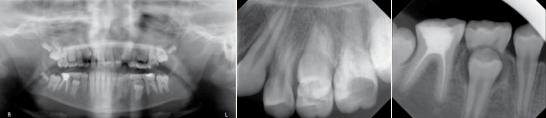
Radiographic investigations were done including (OPT and PA radiographs) to assess the proximity of the coronal defect to the pulp and to evaluate the periapical region and to ascertain the presence and stage of development of remaining permanent dentition (especially lower 7s, 5s and 8s).
MIH was diagnosed based on clinical appearance. See Figures 1 (a, b, c, d & e) for clinical features. Figures 2 (a, b & c) for radiographic findings.A diagnostic list and treatment plan was formulated by a specialist of Paediatric dentist as well as orthodontist and explained in detailed to the father.
Fig. 1 (a, b, c, d & e). Showing a dislodged filling of 36. 16 yellowish brown hypomineralised lesions. 36 and46 large composite fillings.
Fig. 2 (a, b & c). OPT radiograph showing: normal alveolar bone levels, a normally developing dentition, except lower left third molar, E’s are near physiological exfoliation, more than 2/3 of the roots of 7’s are calcified, 46 RCT’ed, 36 composite restoration, 16.26 deep caries. PA radiograph showing: no signs of perapical radiolucency in lower and upper left first molars.
Fig. 3 (a, b, c, d & e). Immediate post- treatment completion images. All first permanents molar were restored with SSCs. Good gingival health and oral hygiene were noted.
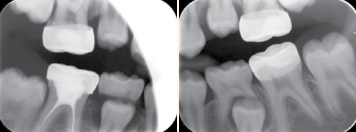
Fig. 4 (a & b). Bitewing radiographs taken 6 months post treatment completion .Radiographic finding, fully seated crowns of all first permant molars with no progression of any pathological lesion underneath the SSC.
Diagnostic Summary
A fit and healthy 10-year-old girl in the late mixed dentition with molar incisor hypomineralisation (MIH). MIH was diagnosed based on clinical appearance.
Aims and objectives of treatment
• To alleviate the pain and sensitivity.
• To preserve the structure of the weakened FPMs.
• To formulate an individualized realistic preventive scheme and reinforce it regularly.
• To monitor the occlusion of developing dentition and treat as necessary.
• Maintain good oral health in the long term.
Treatment Plan Short /medium term
• Emergency phaseo Sedative filling of 26
• Preventive care phaseo Oral hygiene instructionso Diet analysis and adviceo Plaque scoreo Fluoride advice
• Restorative treatment phaseo Stainless steel crowns for all permanent first molars
• Recall and reviewso Regular recall 3 months, radiographs every 6 months and fluoride varnish application every 3 months
Treatment Plan Medium / long term
• Monitor the eruption of permanent dentition
• Interdisciplinary management
Treatment
The treatment plan was set in two phases including Short/Medium term and long term. The short term will start with Emergency phase for restoring the 26 with GI as a temporary filling. An extensive preventive programme was implemented to improve SS’s oral hygiene in addition to diet assessment, analysis, and advice and fluoride application. In several visit crown preparation was done under local anesthesia for 36, 46, 16, and 26 followed by stainless steel crown placement. Patient’s occlusion was checked for any discrepancy in each visit.
As S.S’s is considered to be of high caries risk status .She was kept on regular recall programme including recall visits and fluoride varnish application every 3 months, radiographs every 6 months. See Figures 3 (a, b, c, d & e).
Long Term Treatment Plan and Future Considerations
• Regular long-term diet monitoring and reinforcement of oral hygiene practices.
• Periodic review of the restorations with radiographic assessment.
• Review the first permanent molars status.
• Monitor eruption and development of dentition.
• Educate patient and parents about the poor long-term prognosis of first permanent molars these teeth and available future treatment options.
Discussion
Children with MIH have higher treatment needs and significant challenges in behaviour management than other children. S.S was a quiet girl who was apprehensive in the beginning of the dental treatment but willing to have the treatment. S.S was diagnosed as MIH in first permanent molars. Using non-pharmacological behaviour management techniques including tell-show-do, distraction helped to acclimatize S.S to dental treatment. These techniques are widely used in children’s dentistry and well accepted by parents. The technique works well combined with behaviour shaping. S.S was rewarded with a gift after each appointment as positive reinforcement for her good behaviour and cooperation.26 was temporized with glass ionomer to relief discomfort, stabilize the situation and to reduce bacterial count present in the oral cavity.
Failure of achieving complete anaesthesia of first permanent molars was related to the nature of MIH. S.S received supplemental intralegmental infiltration. The innervations density in the pulp of hypomineralised molars is significantly greater than of normal molars. This can explain why lower left 6 was hard to be anaesthetised. Due to poor quality of the FPM teeth of S.S and significant tooth break down full coverage by preformed metal crowns was done. Preformed metal crowns prevent further tooth loss, control sensitivity, establish correct interproximal and proper occlusal contacts, are not costly and require little time to prepare and insert.
Conclusions
• The presence of MIH molars not only requires the dentist to identify problems at the earliest opportunity, but also to clarify the problem thoroughly and explain the treatment options to the parents and child.
• It is advisable to consider children with a poor general health in the first four years after birth at risk for MIH. These children should be monitored more frequently during eruption of the first permanent molars.
• Whilst many potential approaches exist for the restorative management of molar incisor hypomineralisation, few are yet supported by good quality clinical research data. Preformed Metal crowns have been recommended as the prosthesis of choice in MIH afflicted posterior teeth with post-eruptive enamel breakdown in majority of the literature available.
• The use of nitrous oxide inhalation sedation can be a useful adjunct in obtaining satisfactory analgesia in MIH patients. Nitrous oxide was not used in the case of S.S. due to parental refusal because of limited financial resources.
• Had this patient presented earlier, consideration for enforced extraction of FPM would have been considered.
References
1. Weerheijm KL. Molar incisor hypomineralization (MIH): clinical presentation, aetiology and management. Dent Update. 2004;31(1):9–12.
2. Weerheijm KL, Duggal M, Mejàre I, Papagiannoulis L, Koch G, Martens LC, et al. Judgement criteria for molar incisor hypomineralisation (MIH) in epidemiologic studies: a summary of the European meeting on MIH held in Athens, 2003. Eur J Paediatr Dent. 2003;(4):110–3.
3. Beentjes V, Weerheijm KL, Groen HJ. Factors involved in the aetiology of molar-incisor hypomineralisation (MIH). Eur J Paediatr Dent. 2002;3:9–13.
4. Willmott NS, Bryan RAE, Duggal MS. Molar-incisor-hypomineralisation: a literature review. Eur Arch Paediatr Dent. 2008;9(4):172–9.
5. Seale NS, Randall R. The Use of Stainless Steel Crowns: A Systematic Literature Review. Pediatr Dent. American Academy of Pediatric Dentistry; 2015;37(2):145–60.
6. Lygidakis NA. Treatment modalities in children with teeth affected by molar-incisor enamel hypomineralisation (MIH): a systematic review. Eur Arch Paediatr Dent. 2010;11(2):65–74.
7. Cobourne MT, Williams A MRA. Guideline for the Extraction of First Permanent Molar In Children. (revised 2014). www.rcseng.ac.uk/fds/publications-clinical guidelines/clinical_guidelines. 2014.
One thought on “Clinical Management Approach of Molar Incisor Hypomineralisation. A case report.”
In this article Dr. Thomas Zumstein presents a Neoss implant case that has been in function for more than 11 years. The case shows that long-term success ...
Ectopic eruption of the first permanent molar occurs due to the abnormal mesioangular eruption path of the molar resulting in an impaction at the distal ...
Female patient, 47 years old, presented with a clinical picture of extensive iatrogenic perforation of the furcation region of the dental element 36 (Figs. ...
Implant dentistry has evolved dramatically in the 50 years since Branemark’s first patient was treated. The combination of improved micro-roughened ...
As an oral surgeon and prosthodontist specialising in full-mouth rehabilitation, I have consistently sought to integrate advanced technologies into my ...
Monitoring the developing dentition is part and parcel of a general dental practitioner’s (GDP) routine and this relies on the basic knowledge of tooth ...
A 28-year-old female patient had the primary complaint of spacing in the upper front tooth region. The patient’s medical history did not reveal any ...
Though many smile design programmes offer us solutions for rendering of multiple-tooth replacements, very often in our daily practice we encounter major ...
Polymer-based dental materials, oral care products and routine clinical procedures may all contribute to the release of microplastics and nanoplastics, but ...
Education
Live webinar Tue. 4 August 2026 4:00 am UAE (Dubai)
AJMAN, UAE: Artificial intelligence (AI) is reshaping dental education by changing how students learn, educators teach and institutions prepare graduates ...
BAŞISKELE, Turkey: While traditional behaviour guidance techniques continue to play an essential role in managing anxiety and uncooperative behaviour in ...
JERUSALEM: Infertility is a major reproductive health concern worldwide, and a substantial proportion of cases have no clear explanation. Chronic oral ...

 International / International
International / International
 Brazil / Brasil
Brazil / Brasil
 Canada / Canada
Canada / Canada
 Latin America / Latinoamérica
Latin America / Latinoamérica
 USA / USA
USA / USA
 Austria / Österreich
Austria / Österreich
 Bosnia and Herzegovina / Босна и Херцеговина
Bosnia and Herzegovina / Босна и Херцеговина
 Bulgaria / България
Bulgaria / България
 Croatia / Hrvatska
Croatia / Hrvatska
 Czech Republic & Slovakia / Česká republika & Slovensko
Czech Republic & Slovakia / Česká republika & Slovensko
 France / France
France / France
 Germany / Deutschland
Germany / Deutschland
 Greece / ΕΛΛΑΔΑ
Greece / ΕΛΛΑΔΑ
 Hungary / Hungary
Hungary / Hungary
 Italy / Italia
Italy / Italia
 Netherlands / Nederland
Netherlands / Nederland
 Nordic / Nordic
Nordic / Nordic
 Poland / Polska
Poland / Polska
 Portugal / Portugal
Portugal / Portugal
 Romania & Moldova / România & Moldova
Romania & Moldova / România & Moldova
 Slovenia / Slovenija
Slovenia / Slovenija
 Serbia & Montenegro / Србија и Црна Гора
Serbia & Montenegro / Србија и Црна Гора
 Spain / España
Spain / España
 Switzerland / Schweiz
Switzerland / Schweiz
 Turkey / Türkiye
Turkey / Türkiye
 UK & Ireland / UK & Ireland
UK & Ireland / UK & Ireland
 China / 中国
China / 中国
 India / भारत गणराज्य
India / भारत गणराज्य
 Pakistan / Pākistān
Pakistan / Pākistān
 Vietnam / Việt Nam
Vietnam / Việt Nam
 ASEAN / ASEAN
ASEAN / ASEAN
 Israel / מְדִינַת יִשְׂרָאֵל
Israel / מְדִינַת יִשְׂרָאֵל
 Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس
Algeria, Morocco & Tunisia / الجزائر والمغرب وتونس

 Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
Dr. Cameron Shahbazian DMD MBARegister now1CELive webinar
 Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar
Dr. Bruce McFarlane Certified Specialist in Orthodontics Fellow: Royal College of Dentists of Canada Diplomate: American Board of OrthodonticsLive webinar


 Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
Prof. Dr. Wael Att, Dr. Andrea Laureti ITI Scholar Michigan, Dr. Acela MartinezLive webinar
 Cat EdneyRegister now1CE
Cat EdneyRegister now1CE













































may i get these PDF journal, please ?